
Both cardioversion and defibrillation are medical procedures used to correct abnormal heart rhythms (arrhythmias). However, they are utilised in different clinical situations and employ different techniques.
Cardioversion
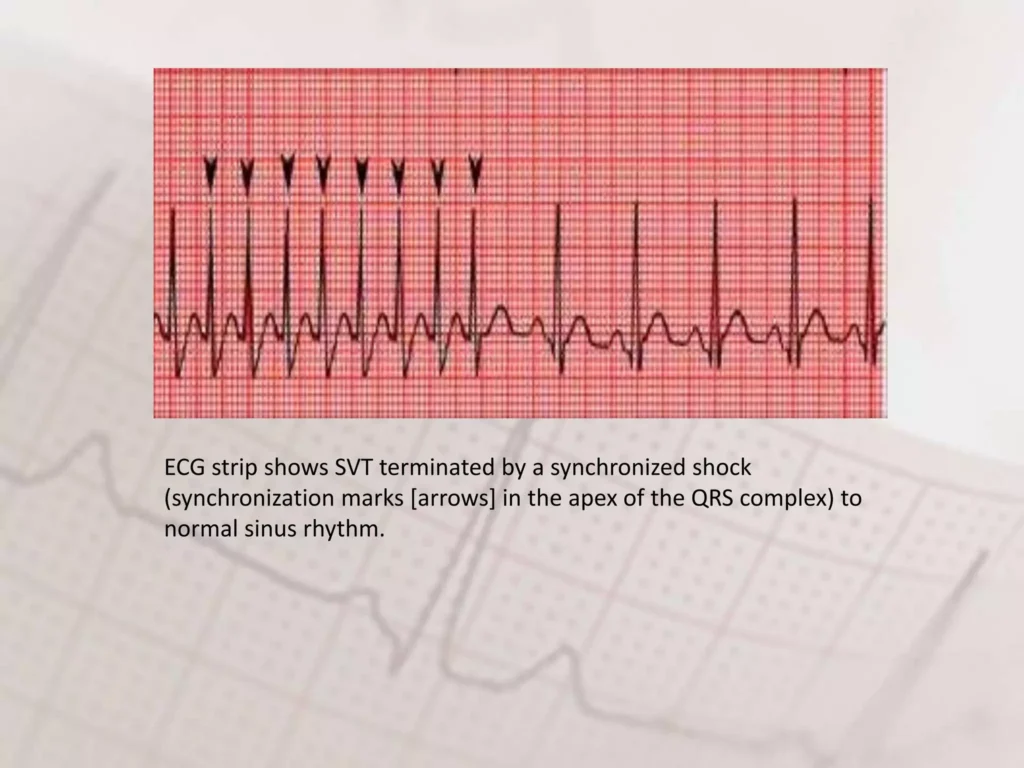
Cardioversion is used to restore a normal heart rhythm in patients with certain types of arrhythmias, such as atrial fibrillation (AF), atrial flutter, and some types of supraventricular tachycardia (SVT). The shock is synchronized with the cardiac cycle, specifically timed with the R wave of the QRS complex, to avoid inducing ventricular fibrillation.
Types of Cardioversion:
- Electrical Cardioversion:
- Procedure: Delivers a synchronised electrical shock to the heart. The shock is timed (synchronised) to coincide with a specific part of the cardiac cycle (usually the R wave of the QRS complex) to avoid causing ventricular fibrillation.
- Setting: Usually performed in a hospital setting under sedation.
- Indications: Used for patients with atrial fibrillation, atrial flutter, and other SVTs that have not responded to medications or other interventions.
- Pharmacological Cardioversion:
- Procedure: Uses antiarrhythemic medications to restore a normal heart rhythm.
- Common Drugs: Amiodarone, flecainide, propafenone, and ibutilide.
- Setting: Can be done in a hospital or sometimes on an outpatient basis.
Indications for Electrical Cardioversion:
- Atrial fibrillation with rapid ventricular response that is not well controlled by medications.
- Atrial flutter.
- Stable but symptomatic SVT that has not responded to vagal manoeuvres or medications.
Complications:
- Risks of thromboembolism, particularly in atrial fibrillation; patients are often anticoagulated before and after the procedure.
- Skin burns at the site of electrode pads.
- Arrhythmias or changes in heart rhythm.
Energy Settings:
- Atrial Fibrillation (AF):
- Initial Shock (Biphasic): 120-150 joules.
- Subsequent Shocks (Biphasic): If the initial shock is unsuccessful, increase to 200 joules.
- Initial Shock (Monophasic): 200 joules.
- Subsequent Shocks (Monophasic): Increase to 360 joules if needed.
- Atrial Flutter and SVT:
- Initial Shock (Biphasic): 70-120 joules.
- Subsequent Shocks (Biphasic): If the initial shock is unsuccessful, increase to 120-150 joules.
- Initial Shock (Monophasic): 50-100 joules.
- Subsequent Shocks (Monophasic): Increase to 200 joules if needed.
Defibrillation
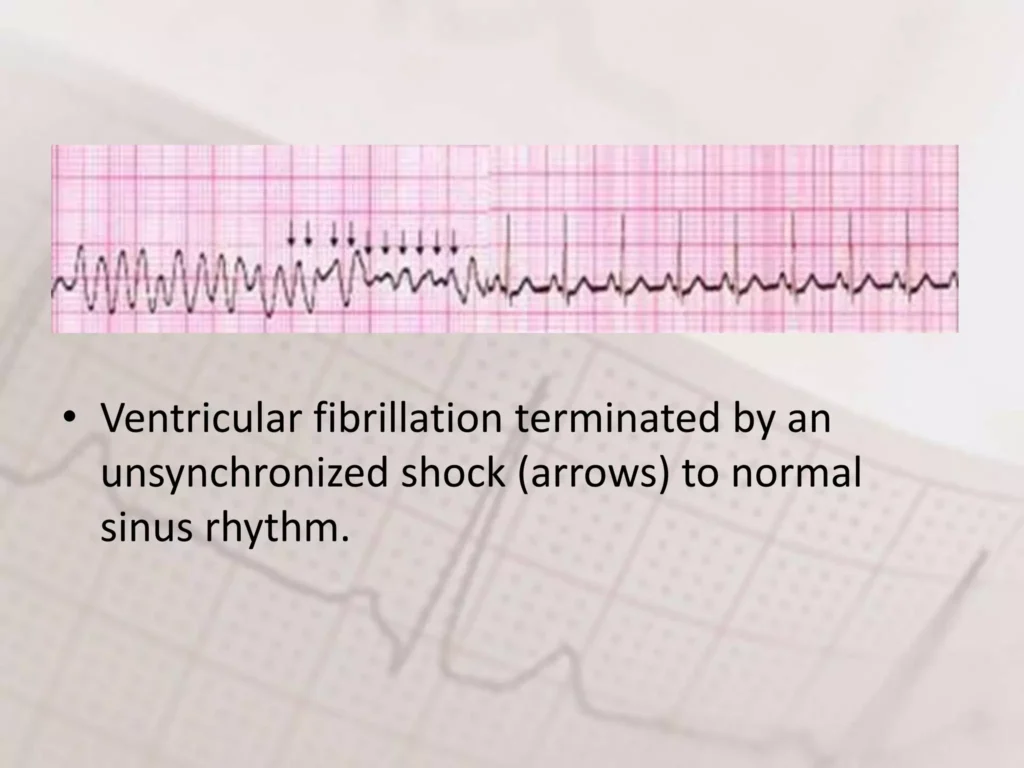
Purpose: Defibrillation is used in emergency situations to treat life-threatening arrhythmias, such as ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT). It is not synchronised with the cardiac cycle.
Procedure:
- Emergency Use: Delivers an unsynchronised electrical shock to the heart, which is not timed with the cardiac cycle.
- Equipment: Uses a defibrillator, which can be external (manual or automated external defibrillators (AEDs)) or internal (implantable cardioverter-defibrillators (ICDs)).
- Setting: Typically performed during cardiac arrest situations, either in-hospital, pre-hospital (by emergency medical services), or by bystanders using AEDs in public places.
Indications:
- Ventricular fibrillation (VF).
- Pulseless ventricular tachycardia (VT).
Complications:
- Skin burns at the site of electrode pads.
- Potential damage to heart muscle, though this is less of a concern in life-threatening situations.
Energy Settings:
- Initial Shock:
- Biphasic Defibrillator: The recommended initial shock is 150-200 joules.
- Monophasic Defibrillator: If using a monophasic defibrillator, the initial shock is delivered at 360 joules.
- Subsequent Shocks:
- Biphasic Defibrillator: If the initial shock is unsuccessful, subsequent shocks are usually delivered at the same or increased energy level, up to 360 joules.
- Monophasic Defibrillator: Subsequent shocks are delivered at 360 joules
Key Differences
| Aspect | Cardioversion | Defibrillation |
|---|---|---|
| Purpose | Treats atrial fibrillation, atrial flutter, and SVTs | Treats life-threatening arrhythmias (VF and pulseless VT) |
| Timing | Synchronized with the cardiac cycle | Unsynchronised |
| Setting | Planned, often elective procedure | Emergency, life-saving procedure |
| Sedation | Performed under sedation | Performed in an emergency, sedation not typically used |
| Energy Levels | Lower energy levels | Higher energy levels |
| Complications | Risk of thromboembolism, arrhythmias | Burns, potential heart muscle damage |