
The Hartmann procedure is named after French surgeon Henri Albert Hartmann, who first described it in 1921. Hartmann developed the procedure in response to the high mortality rate associated with the abdomino-perineal resection described by Miles in 1908. The procedure is a type of colectomy, which means that part of the colon is removed, and is often preferred in emergency cases.

Hartmann’s Procedure: Detailed Overview
Hartmann’s procedure (proctosigmoidectomy) is a surgical operation primarily used to treat diseases and conditions affecting the distal colon, rectum, or sigmoid colon, often in emergency situations. This procedure involves the resection of a diseased segment of the bowel, creation of a colostomy, and closure of the rectal stump.
Indications
Hartmann’s procedure is typically indicated for:
- Colon cancer (Colorectal Cancer) :This is the most common reason for a Hartmann procedure. It’s often used when cancerous tumours are located in the lower part of the colon (sigmoid colon) or rectum. Obstructive or perforated cancer of the distal colon or rectum.
- Complicated Diverticulitis: Acute diverticulitis with perforation, abscess, or fistula formation.
- Ischaemic Bowel Disease: Bowel infarction due to compromised blood supply.
- Traumatic Injury: Severe injury to the colon requiring resection.
- Infectious Colitis: Severe infections leading to bowel perforation.
- Ulcerative colitis: In severe cases of ulcerative colitis, a chronic inflammatory bowel disease
Surgical Procedure
1. Preoperative Preparation
- Assessment: Detailed medical history, physical examination, and imaging studies (CT scan, colonoscopy) to determine the extent of disease.
- Stabilisation: Managing sepsis, dehydration, and correcting electrolyte imbalances if necessary.
- Consent: Obtaining informed consent after discussing risks, benefits, and alternatives.
2. Anaesthesia
- General anaesthesia is administered for the procedure.
3. Surgical Steps
- Incision: A midline laparotomy or a lower abdominal incision is made.
- Exploration: The abdomen is explored to assess the extent of the disease.
- Resection: The affected segment of the colon is identified and resected.
- Colostomy: The proximal end of the bowel is brought out through the abdominal wall to form a colostomy.
- Rectal Stump Closure: The distal stump of the rectum is closed and left in situ. During a colostomy, the surgeon cuts the bowel and brings one end out onto the abdominal wall as a stoma, while the other end is sewn or stapled closed. The closed end is called the rectal stump
- Drain Placement: Drains may be placed near the rectal stump to prevent fluid accumulation.
4. Postoperative Care
- Monitoring: Vital signs, fluid balance, and stoma function are closely monitored.
- Pain Management: Analgesics are administered to manage postoperative pain.
- Antibiotics: Continued use of antibiotics to prevent or treat infection.
- Nutrition: Gradual reintroduction of diet, starting with clear liquids and progressing to solid foods as tolerated.
- Stoma Care: Education on stoma care and management is provided to the patient and caregivers.
Complications
Potential complications of Hartmann’s procedure include:
- Infection: Surgical site infection, intra-abdominal abscess.
- Bleeding: Postoperative bleeding or haematoma formation.
- Anastomotic Leak: Leak from the rectal stump closure.
- Stoma Complications: Stoma prolapse, retraction, or skin irritation.
- Bowel Obstruction: Adhesions or strictures leading to bowel obstruction.
- Deep Vein Thrombosis (DVT): Increased risk due to immobility and surgery.
Reversal of Hartmann’s Procedure
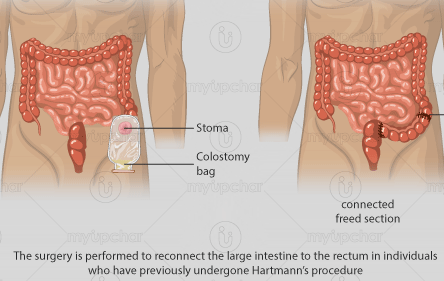
A second operation, known as Hartmann’s reversal or colostomy takedown, can be performed to restore bowel continuity. This is typically considered after the patient has fully recovered from the initial surgery and any inflammation or infection has resolved.
Timing:
- Usually performed 3-12 months after the initial procedure, depending on patient recovery and overall health.
Procedure:
- Laparotomy: An abdominal incision is made to access the bowel.
- Colostomy Takedown: The colostomy is reversed, and the proximal end is reconnected to the rectal stump.
- Anastomosis: A primary anastomosis is created to restore bowel continuity.
Postoperative Care:
- Similar to the initial procedure, with close monitoring of anastomosis integrity, bowel function, and management of potential complications.
Conclusion
Hartmann’s procedure is a critical surgical intervention for managing severe colorectal conditions, especially in emergency situations. While it can be lifesaving, it comes with potential risks and complications. Comprehensive preoperative assessment, meticulous surgical technique, and diligent postoperative care are essential for optimal outcomes. The possibility of reversal offers patients a chance to restore normal bowel function once they have recovered from the initial surgery.